Hormone Therapy for Breast Cancer: What you should know!
Hormone therapy for breast cancer, often called maintenance therapy, is an important treatment option for women with hormone-dependent breast cancer. It can inhibit or stop the growth of tumor cells that respond to estrogen or progesterone. Hormone therapy can be used as an adjunct to surgery, chemotherapy, or radiation to reduce the risk of relapse or progression of the disease. It can also be used in advanced breast cancer to relieve symptoms or improve quality of life. In this article, you will learn more about the different forms of hormone therapy (also called maintenance therapy), monitoring with maintrac, and how to know when it is safe to stop the maintenance therapy.

What Forms of Hormone Therapy for Breast Cancer are there?
There are various drugs that can block the formation or effect of estrogens. The choice of drug depends on various factors such as the age of the patient, menstrual status, hormone receptor status of the tumor, and previous therapy. The most important groups of drugs are:
Hormone Therapy for Breast Cancer with Anti-Estrogens:
These drugs bind to the hormone receptors of tumor cells and thus prevent estrogen from docking onto them. The best-known anti-estrogen is tamoxifen, which can be used in both premenopausal and postmenopausal women. Tamoxifen is usually taken as a tablet and has a duration of action of about 24 hours.
Aromatase Inhibitors:
These drugs inhibit the enzyme aromatase, which produces estrogens from other hormones in fat and muscle tissue. Aromatase inhibitors are only effective in postmenopausal women because they do not affect estrogen production in the ovaries. They are usually taken as a tablet and have a duration of action of about 48 hours. There are three aromatase inhibitors: anastrozole, letrozole, and exemestane.
GnRH Analogues:
These drugs are synthetic variants of the natural hormone GnRH that controls the release of estrogen and progesterone from the ovaries. GnRH analogues suppress ovarian function and thus induce artificial menopause. They are usually administered as an injection under the skin and have a duration of action of about four weeks. They are often given in combination with an aromatase inhibitor or an anti-estrogen to achieve maximum effect.
Fulvestrant:
This drug is a special anti-estrogen that not only binds to hormone receptors but also destroys them. Fulvestrant is administered as an injection into muscle and has a duration of action of about four weeks. It is usually used in advanced breast cancer when other hormone therapies no longer work.
How is Hormone Therapy for Breast Cancer Monitored?
Maintenance therapy is usually carried out over a period of at least five to ten years. To assess the success of therapy and detect possible side effects, regular monitoring is necessary. This includes:
Clinical examinations:
The patient should regularly visit her doctor to have her general condition, breast, and lymph nodes examined. She should also watch for possible signs of thrombosis (blood clot), endometriosis (overgrowth of the uterine lining), or uterine cancer, which can occur as rare but serious side effects of some hormone therapies.
Blood tests:
The patient should regularly have her blood count, liver values, and bone metabolism checked to detect possible changes due to hormone therapy. She should also have her cholesterol level and blood pressure monitored, as some hormone therapies can increase the risk of cardiovascular disease.
Imaging procedures:
The patient should regularly undergo mammography (X-ray examination of the breast) and, if necessary, sonography (ultrasound examination of the breast) to detect possible changes in the breast. However, tumors are often already about 1 cm in diameter before they are detected. In addition, she should have a bone density measurement (osteodensitometry) if necessary to prevent or treat possible bone loss due to hormone therapy for breast cancer.
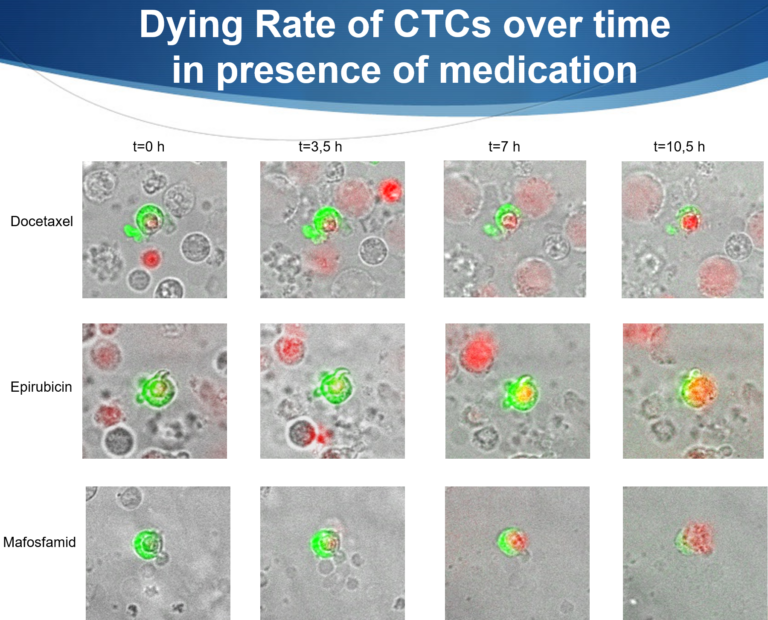
maintrac:
This is a special procedure that determines the number and properties of circulating tumor cells in the blood. Circulating tumor cells are cancer cells that have detached from the primary tumor or metastases and circulate in the bloodstream. They can serve as markers for response or progression of the disease. With maintrac, you can monitor the effect of hormone therapy on circulating tumor cells and thus adjust therapy very early and individually.
When can Hormone Therapy be Stopped?
The duration of hormone therapy depends on various factors. As example such as the age of the patient, the stage of the disease, the hormone receptor status of the tumor, and response to therapy. Hormone therapy is generally recommended for at least five years. It significantly reduces the risk of relapse or progression of the disease. However, for some patients it may be useful to continue maintenance therapy for longer, for example if:
• The tumor is strongly hormone-dependent: If the tumor has a high proportion of hormone receptors, it usually responds well to hormone therapy and has a lower risk of relapse. Longer hormone therapy can enhance this effect and improve survival.
• The tumor has multiple risk factors such as large size, high degree of malignancy, lymph node involvement or HER2-positive status, it has a higher risk of relapse or progression of disease. Longer hormone therapy can reduce this risk and improve survival.
• The patient has no severe side effects: If the patient tolerates hormone therapy well and has no severe side effects, she may benefit from a longer duration of therapy. However, side effects should be regularly monitored and treated.
Duration of Maintenance Therapy
The decision on the duration of hormone therapy should be made individually with the doctor. Please take into account the advantages and disadvantages of a longer or shorter therapy. The maintrac procedure should also be used to assess the effect of the maintenance therapy on circulating tumor cells. If the number of circulating tumor cells is stable or decreasing during hormone therapy, this indicates a good effect of hormone therapy. However, if they increase, this indicates resistance or progression of the disease. In this case, hormone therapy should be changed or adjusted.
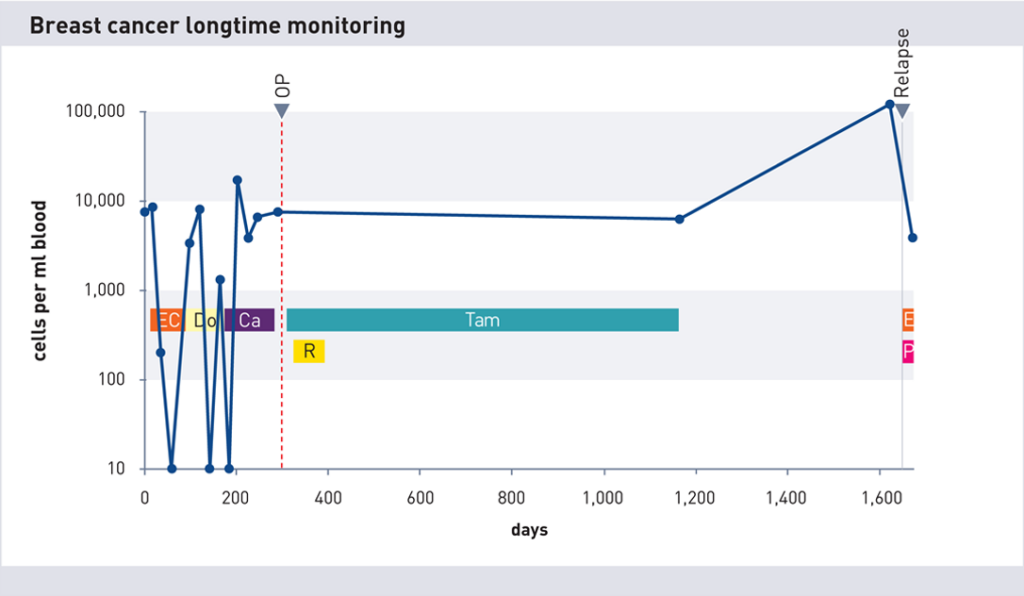
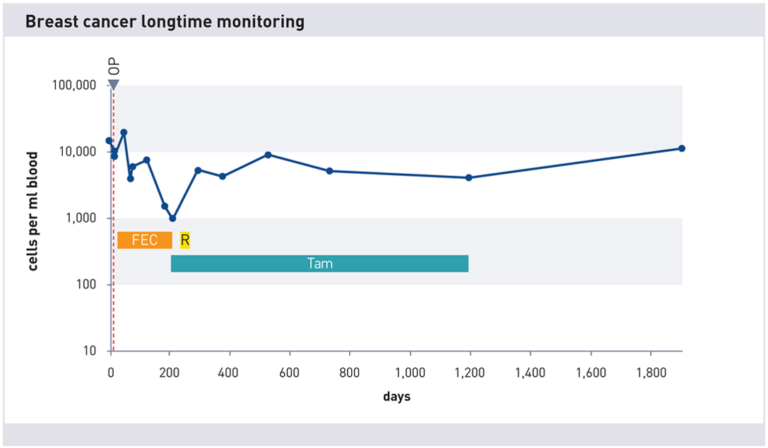
After stopping tamoxifen therapy (~Day 1180), the cell count increases significantly (factor 10). Shortly thereafter, recurrence detected by imaging.
At the End of Hormone Therapy
When tamoxifen or aromatase inhibition therapy is to be discontinued, it is recommended to perform at least 3 cell counts during therapy and measure the cell count again 8-12 weeks after the end of therapy. If the cell count has remained the same or decreased, this is a good sign and it is recommended to monitor the cell count at intervals of 6-9 months. However, if the cell count has increased by a factor of about 3 or more, then hormone therapy should be resumed. In one study, patients with significantly increasing numbers developed a recurrence 9-12 months later.
Conclusion
Hormone therapy proves to be life-saving for thousands of women every year. However, it is hardly possible for the doctor to predict whether it is safe to stop therapy. This is where the maintrac method comes into play and can predict new tumor activity very early on in most cases through significantly increasing tumor cell counts.
Please note that this article is for informational purposes only and does not replace consultation or treatment by a doctor.